
Isolated CNS leukaemic relapse in acute myeloid leukaemia:
Description
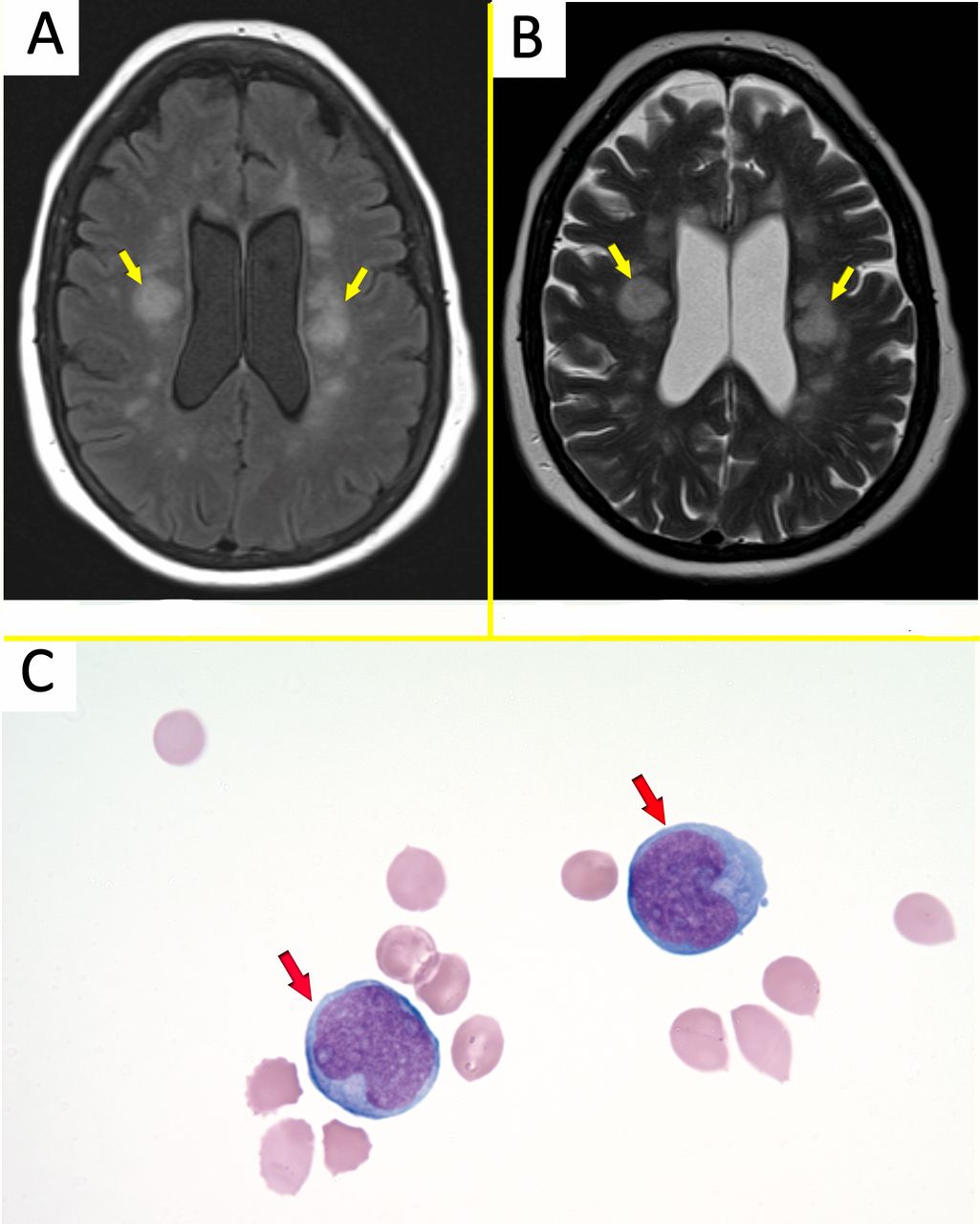
A 61-year-old woman with acute myeloid leukaemia (AML) without maturation (M1) with trisomy 13 who achieved complete remission after her initial diagnosis with cytarabine and idarubicin. Two years later, she relapsed and underwent successful haematopoietic stem cell transplantation afterwards, and she entered complete remission. Sixteen months later, she presented to our emergency department with a 2-week history of worsening fatigue, progressive expressive aphasia and then she lapsed coma. On the workup, there was no identifiable reversible metabolic or infectious cause of her presentation. Brain MRI revealed multifocal patchy abnormalities in the white matter (figure 1A,B). Her lumbar puncture (LP) revealed blasts on the cytocentrifuge preparations of cerebrospinal fluid (CSF) (figure 1C). Flow cytometry on the CSF confirmed the presence of a myeloblast population with 14% blasts with expression of CD13, CD33, CD34, CD45 and Human Leukocyte Antigen – DR isotype (HLADR). And fluorescence in situ hybridization test was negative for Promyelocytic Leukemia/Retinoic Acid Receptor alpha (PML/RARa) translocation. There was no evidence of blast cells on the peripheral blood smear. And, bone marrow aspirate and biopsy revealed no evidence of blasts, indicating isolated central nervous system (CNS) relapse as the patient had no signs of other extramedullary involvement manifestation. Despite treatment with intrathecal methotrexate, she continued to deteriorate and died.

Download figure
{kind=link}
Open in new tab
{kind=link}
Download powerpoint
Figure 1
(A,B) Brain MRI T2 weighted sequence showing periventricular flair and hyperintensity (yellow arrows) with multifocal patchy abnormalities in the white matter characterised as restricted diffusion. (C) Cerebrospinal fluid showing large cells with increased nuclear size, increased nuclear/cytoplasmic ratio, fine chromatin and prominent nucleoli, consistent with blasts (red arrows).
CNS complication in patients with leukaemia can be related to several mechanisms; direct involvement, vascular complications and infectious complications related to the disease itself or the treatment. CNS involvement in adults with AML is less common when compared with acute lymphoblastic leukaemia and is rare in general, and routine evaluation for CNS involvement is not recommended in absence of CNS symptoms.1 Symptoms of CNS involvement depends generally on the involved anatomy and pathology. LP should be the initial workup for suspected CNS involvement and identification of leukaemic blasts on CSF should confirm the diagnosis.2 CNS imaging studies should be performed based on the manifestations and to exclude other suspected possible pathology (eg, stroke, inflammatory or vascular lesions). Treatment include intrathecal chemotherapy and radiation therapy. Particular clinical features associated with a higher risk for CNS involvement in AML have been reported in the literature.1 3
We thought the MRI finding, in this case, was related to myeloid sarcoma in the setting of isolated CNS leukaemic relapse. Myeloid sarcoma is a term for a tumour mass of myeloblast or immature myeloid cells occurring in an extramedullary site or the bone.4
This case demonstrates a good example of CNS imaging in CNS leukaemic relapse that can be an instructive case for other clinicians. Also, it highlights the importance of imaging and pathology along with other clinical data in yielding the final diagnosis.
Learning points
Central nervous system (CNS) involvement in acute myeloid leukaemia is rare compared with acute lymphoblastic leukaemia.
Lumbar puncture with cerebrospinal fluid analysis for blasts should be the initial workup once CNS involvement is suspected.
CNS imaging should be directed towards a specific clinical presentation, and it can aid in the diagnosis.
References
↵
Alakel N ,
Stölzel F ,
Mohr B , et al . Symptomatic central nervous system involvement in adult patients with acute myeloid leukemia. Cancer Manag Res 2017;9:97–102.doi:10.2147/CMAR.S125259
Google Scholar
↵
Arber DA ,
Borowitz MJ ,
Cessna M , et al . Initial diagnostic workup of acute leukemia: guideline from the College of American pathologists and the American Society of hematology. Arch Pathol Lab Med 2017;141:1342–93.doi:10.5858/arpa.2016-0504-CP
Google Scholar
↵
Shihadeh F ,
Reed V ,
Faderl S , et al . Cytogenetic profile of patients with acute myeloid leukemia and central nervous system disease. Cancer 2012;118:112–7.doi:10.1002/cncr.26253
CrossRefPubMedGoogle Scholar
↵
Jaffe ES ,
Harris NL ,
Stein H , et al.
Brunning RD ,
Bennett J ,
Matutes E . Acute myeloid leukemia not otherwise categorised. In: Jaffe ES , Harris NL , Stein H , et al. , eds. Who classification of tumours; pathology and genetics of tumours of haematopoietic and lymphoid tissues. Lyon: IARC Press, 2001: 104–5.
Google Scholar
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου