
Original Research
9 (
165-171
3
); 165-171
doi:
10.25259/APOS_23_2019
Skeletal and dental changes after lower posterior tooth extrusion in Class II Division 1 deep bite short-faced growing patients
Pornpan Jariyavithayakul, Chairat Charoemratrote
Department of Preventive Dentistry, Faculty of Dentistry, Prince of Songkla University, Hat Yai, Songkhla, Thailand

Published: 2019-09-28,
Accepted: 2019-04-24,
Received: 2019-03-20
How to cite this article: Jariyavithayakul P, Charoemratrote C. Skeletal and dental changes after lower posterior tooth extrusion in Class II Division 1 deep bite short-faced growing patients. APOS Trends Orthod 2019;9(3):165-71.
Accepted: 2019-04-24,
Received: 2019-03-20
© 2019 Published by Scientific Scholar on behalf of APOS Trends in Orthodontics
Licence
This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
How to cite this article: Jariyavithayakul P, Charoemratrote C. Skeletal and dental changes after lower posterior tooth extrusion in Class II Division 1 deep bite short-faced growing patients. APOS Trends Orthod 2019;9(3):165-71.
Abstract
Objectives:
The objectives of the study were to investigate the effect of lower posterior tooth extrusion on skeletal and dental changes in Class II division 1 deep bite short-faced growing patients.Materials and Methods:
Twenty-two growing patients with Class II/1 malocclusion deep bite/short-face were treated using a pre-adjusted edgewise-fixed appliance. The curve of Spee (COS) was leveled by rectangular wire and posterior vertical elastic. Two consecutive lateral cephalometric radiographs were collected before and after treatment. Changes from the cephalometric analysis were compared with 22 untreated matched subjects during the observation period with independent t-test.Results:
The reduction of deep bite from the COS in the treated group was 2.83 mm which was obtained by a greater amount of posterior extrusion (1.37 mm), than anterior intrusion (0.58 mm), and lower facial height significantly increased (3.70 mm). The treated group showed significant forward mandibular position from SNB (1.36°), Pg-Nperp (1.53 mm), and the skeletal relationship improved (ANB = −0.88°). The mandibular plane angles (SN-MP and FMA) showed no significant changes during treatment. Dental changes revealed significant decreases in overjet and overbite, whereas the position and inclination of the upper and lower incisors were not significantly different.Conclusions:
The increase of lower facial height in Class II deep bite short-faced growing patients was successfully accomplished by lower posterior tooth extrusion with the use of rectangular wire with posterior vertical elastic. The mandibular plane angle did not change during treatment. Class II skeletal relationship improved by the forward position of the mandible in hypo- and normodivergent pattern subjects.Keywords
Class II division 1 malocclusion
Deep bite
Lower posterior tooth extrusion
Dentofacial
INTRODUCTION
Class II malocclusion has been found in 20–30% of all orthodontic patients.[1,2] This type of malocclusion may exhibit various skeletal and dental configurations. Either maxillary protrusion or mandibular retrusion can be the causative factor; however, the most common configuration in a Class II malocclusion is mandibular retrusion.[3] Class II malocclusion usually is perceived as a sagittal problem and also accompanied by vertical concerns.[4]Deep bite is often observed in Class II patients. In growing patients, one modality used to correct Class II deep bite is cervical pull headgear. This application increases the vertical dimension measurement and creates upper molar extrusion.[5] On the other hand, deep bite can be caused by an excessive curve of Spee (COS).[6] It has been reported that the COS was the greatest in Class II malocclusion.[7]
To establish a proper incisal relationship and posterior occlusion in orthodontic patients, the COS must be relatively flat to mild.[8] Excessive COS can be corrected by the anterior intrusion, posterior extrusion or a combination of the two procedures.[9,10] The treatment might involve intrusion of the anterior teeth.[9] However, it has also been suggested that a deep COS should be corrected by extrusion of the molars because intrusion of anterior teeth has a high potential for relapse.[10] Since there is no consensus on this issue, it is necessary to identify the cause before treating an excessive COS.[11] Possible causes of a COS include lack of eruption of posterior teeth, overeruption of the anterior teeth, or a combination of both.
Evaluating lower anterior facial height is also important for decision-making between posterior extrusion and anterior intrusion. In the case of short-faced patients, posterior extrusion leads to opening rotation of the mandible and, consequently, the lower facial height is increased. This improves vertical facial proportions. However, opening rotation of the mandible also leads to a more severe Class II relationship with a worsened convex profile.[12] It was also suggested that the mandible can be restrained by deep overbite. Therefore, in growing patients, the resolution of deep bite might benefit the sagittal discrepancy by unlocking the restrained mandible and allowing its forward growth,[13,14] whether or not this actually occurs remains controversial. The purpose of this study was to determine whether there were differences in the skeletal and dental changes between Class II division 1 malocclusion growing patients treated to level the COS by posterior extrusion and untreated controls.
MATERIALS AND METHODS
This study was approved by the Ethics Committee on human research at the Faculty of Dentistry, Prince of Songkla University (Approval no. MOE 0521.1.03/356). All participants and their parents provided informed consent before participating in this study.Subjects
This was a prospective study. The experimental group consisted of 22 subjects (10 females and 12 males) and the control group was comprised 22 untreated subjects (12 females and 10 males). The inclusion criteria for recruitment into the study were: (1) Skeletal Class II patients (ANB >5°); (2) Class II division 1 malocclusion with bilateral Class II molar relationship; (3) hypo- to normodivergent mandibular plane angle (FMA <27°); (4) decreased lower facial height (lower anterior facial height to total anterior facial height <54%);[15] (5) COS >2 mm; (6) no or mild crowding (<3 mm); (7) growth stage 4–5 on the hand-wrist radiograph according to Björk[16] and Grave and Brown;[17] and (8) no previous history of orthodontic treatment. Subjects excluded from the study were patients with craniofacial disorders, skeletal asymmetry, dysfunctional disorders of the masticatory system or temporomandibular joint, or presenting with abnormal oral habits.The sample size was calculated using the PS Power and Sample Size Calculation software, version 3.0.43 (Vanderbilt University, Nashville, TN, USA) based on the parameter values (L6-MP) taken from a study by Bernstein et al.[18] with a mean difference of 2.31 mm and standard deviation (SD) of 2.28. The levels of significance of the change and power of the test were established at 95% (α = 0.05) and 80% (β = 0.2), respectively. A minimum of 16 patients in each group was required. Twenty-two patients who met the inclusion criteria were assigned to the experimental group. Another 22 subjects who met the same inclusion criteria were assigned to the untreated control group. The subjects in the control group were obtained from two sources of records at the dental hospital: (1) Retrospective records of previously growth-monitored patients who were receiving or had completed orthodontic treatment and (2) treatment records of growing patients who refused treatment with specific reasons but later returned with a new decision to undergo treatment and had not received any orthodontic treatment elsewhere.
Treatment protocol
Leveling and aligning were performed in the experimental group with pre-adjusted edgewise-fixed appliances including 0.018 – in slot brackets on incisors and 0.022 – in slots on the remaining teeth (Roth system; Ormco Corp., Glendora, CA, USA). The initial alignment was achieved using NiTi archwires and stainless steel until 0.016 × 0.016 – in stainless steel wires were placed in the upper arch. In the case of a narrow upper arch, the upper arch was expanded with an expanded form of 0.016 × 0.022 – in TMA wire. Then, stainless steel wire 0.018 × 0.025 – in was maintained in the upper arch.
system; Ormco Corp., Glendora, CA, USA). The initial alignment was achieved using NiTi archwires and stainless steel until 0.016 × 0.016 – in stainless steel wires were placed in the upper arch. In the case of a narrow upper arch, the upper arch was expanded with an expanded form of 0.016 × 0.022 – in TMA wire. Then, stainless steel wire 0.018 × 0.025 – in was maintained in the upper arch.In the lower arch, the procedure was the same as the upper arch. COS leveling was done with step bends at the lower anterior teeth on 0.016 × 0.022 – in stainless steel wire. The archwires used during the leveling stage were cinched. Kobayashi hooks were attached to the upper and lower premolars. Vertical elastics (1/8” 3.5 oz.) were placed between the upper and lower premolars [Figure 1]. Patients were instructed to use the elastics continuously except when eating and brushing their teeth. Post-treatment records were taken after a flattened COS, confirmed by dental cast analysis, was achieved.

Close
Figure 1::
Illustrating the use of vertical elastics.
Illustrating the use of vertical elastics.
Data collection and analysis
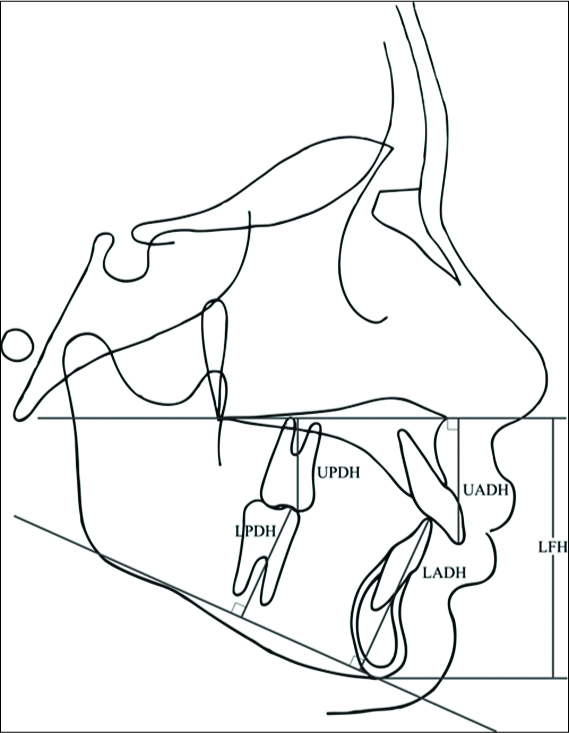
Lateral cephalograms were taken using a Gendex GXDP-700 series (Gendex Dental System, Hatfield, PA, USA). The initial (T0) and post-observation (T1) cephalograms of the untreated control group and pre-treatment (T0) and post-treatment (T1) cephalograms of the treated group were collected. Tracing, registration of the landmarks, and measurements were performed by one examiner blinded to the purpose of the study using Dolphin ImagingPlus 11.7 software (Dolphin Imaging and Management Solutions, Chatsworth, CA, USA). All cephalograms were standardized and all measurements were adjusted for magnification. The cephalometric measurements are detailed in Table 1 and Figure 2.Table 1:: Cephalometric distances and angles used for the analysis.
| Skeletal measurements | Definition |
| SNA° | Angle between sellanasion point A |
| SNB° | Angle between sellanasion point B |
| ANB° | Angle between point Anasion-point B |
| ANperpmm | Distance from point A to Nperpendicular |
| PgNperpmm | Distance from pogonion to Nperpendicular |
| SNMP° | Angle between sellanasion plane and mandibular plane (plane tangent to gonial angle and gnathion) |
| FMA° | Angle between Frankfort horizontal plane and mandibular plane (plane tangent to the lower border of the mandible and the lowest point at symphysis) |
| LFHmm (lower facial height) | Distance from anterior nasal spine to menton |
| Dental measurements | Definition |
| U1-NA° | Angle between axial inclination of maxillary incisors and the line from nasion to point A |
| U1-NAmm | Distance between incisal tip of maxillary incisors and the line from nasion to point A |
| L1-NB° | Angle between axial inclination of mandibular incisors and the line from nasion to point B |
| L1-NBmm | Distance between incisal tip of mandibular incisors and the line from nasion to point B |
| U1-L1° | Interincisal angle (angle between axial inclination of maxillary and mandibular incisors) |
| U1-PP° | Angle between axial inclination of maxillary incisor and the palatal plane (line connecting anterior and posterior nasal spine) |
| L1- MP° | Angle between axial inclination of mandibular incisor and the mandibular plane (plane tangent to gonialangle and the lowest point at symphysis) |
| Overjetmm | Horizontal overlapping distance from the incisal edge of maxillary incisors to labial surface of mandibular incisors |
| Overbitemm | Vertical overlapping distance of maxillary and mandibular incisal edges |
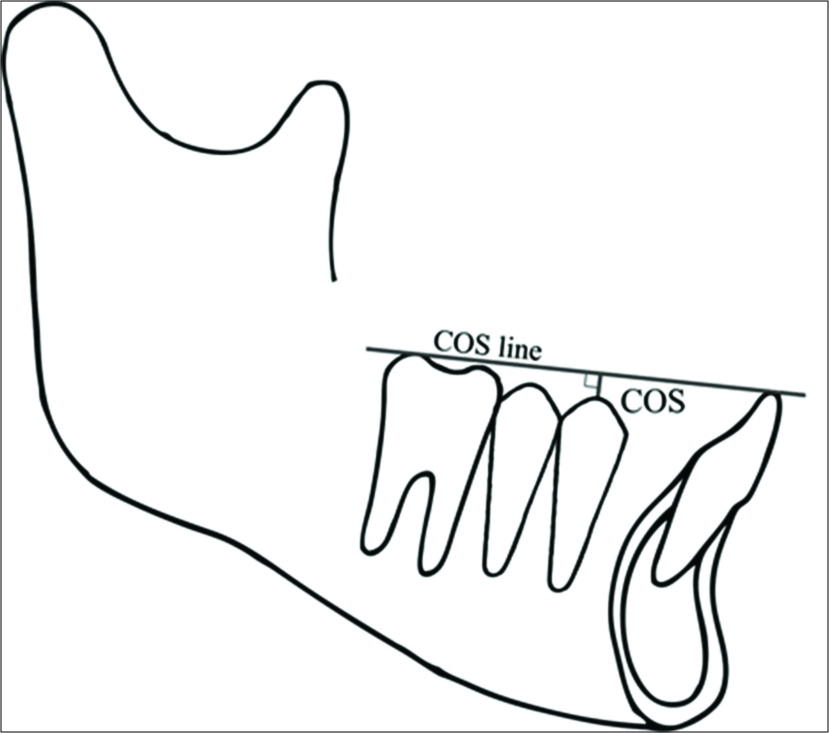
| Curve of Speemm (COS) | The perpendicular distance between the deepest cusp tip and a flat plane between incisal edges of the central incisors and the distal cusp tips of the most posterior teeth in the lower arch |
| UADHmm (Upper anterior dental height) | The perpendicular distance from the upper incisal edge projected to the palatal plane |
| UPDHmm (Upper posterior dental height) | The perpendicular distance from the mesiobuccal cusp tip of the first upper molar to palatal plane |
| LADHmm (Lower anterior dental height) | The perpendicular distance from the lower incisal edge to the mandibular plane |
| LPDHmm (Lower posterior dental height) | The perpendicular distance from the mesiobuccal cusp tip of the first lower molar to the mandibular plane |
Close
Figure 2::
Lower facial height and dental height measurements.
Lower facial height and dental height measurements.
Close
Figure 3::
Measurement of the depth of the curve of Spee.
Measurement of the depth of the curve of Spee.
Method error
Method errors in locating landmarks and measurements were assessed using Dahlberg’s formula.[20] 15 randomly selected radiographs each from T0 and T1 were re-measured by the same examiner at an interval of 2 months. Linear and angular measurements did not exceed 0.5 units for any of the variables investigated.Statistical analysis
All statistical analyses were performed using SPSS 17.0 for Windows software (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05 for all tests. The differences in sex within each group were also examined with independent t-test. Since there were no significant differences in the values between male and female subjects, they were considered as a whole for subsequent analysis. Initial cephalometric values and treatment changes were reported as means and SDs. Normality was tested using the Shapiro–Wilk test. Independent t-test or Mann–Whitney U-test for non- normally distributed data was used to compare initial values and treatment changes between the groups.RESULTS
Twenty-two patients in the treated group (10 females and 12 males) and 22 patients in the untreated control group (12 females and 10 males) were analyzed. The initial mean (±SD) ages of the subjects were 11.35 ± 0.97 years in the treated group and 11.44 ± 0.87 years in the control group. The mean (±SD) duration of treatment was 0.92 ± 0.21 years and the mean (±SD) observation period for the untreated control group was 0.96 ± 0.12 years [Table 2]. The initial cephalometric values (T0) are presented in Table 3 and showed no significant differences between the groups.Table 2:: Demographic data for treated and untreated control groups.
| Groups | Age at T0 (years) | T0–T1 interval (years) |
|---|---|---|
| Mean±SD | Mean±SD | |
| Treated group | 11.35±0.97 | 0.92±0.21 |
| Untreated control group | 11.44±0.87 | 0.96±0.12 |
| Significance | NS | NS |
NS indicates not significant, P>0.05, SD: Standard deviation
Table 3:: Cephalometric values of pre-treatment (T0) for the treated group and initial record for untreated control group.
| Measurement | Treated | Control | P value |
|---|---|---|---|
| Mean±SD | Mean±SD | ||
| SNA° | 83.70±3.64 | 83.90±3.41 | NS |
| SNB° | 77.39±3.15 | 77.28±3.68 | NS |
| ANB° | 6.31±2.09 | 6.62±2.45 | NS |
| ANperpmm | 1.51±2.93 | 2.00±3.34 | NS |
| PgNperpmm | −8.44±6.40 | −8.56±6.89 | NS |
| SNMP° | 32.69±4.97 | 32.56±5.57 | NS |
| FMA° | 23.15±2.51 | 22.64±3.08 | NS |
| LFHmm | 61.76±4.48 | 62.85±3.90 | NS |
| U1NA° | 27.01±9.12 | 27.47±6.82 | NS |
| U1NAmm | 7.30±3.17 | 6.58±2.49 | NS |
| L1NB° | 30.28±5.25 | 30.61±5.29 | NS |
| L1NBmm | 7.67±2.02 | 7.56±2.03 | NS |
| U1L1° | 115.96±8.81 | 114.13±7.45 | NS |
| U1PP° | 119.78±8.86 | 119.23±7.23 | NS |
| L1MP° | 96.52±6.23 | 96.98±4.42 | NS |
| Overjetmm | 8.25±2.47 | 8.74±1.88 | NS |
| Overbitemm | 4.66±1.2 | 4.55±1.05 | NS |
| COSmm | 3.31±0.76 | 3.66±0.82 | NS |
| UADHmm | 28.35±3.33 | 28.23±5.74 | NS |
| LADHmm | 39.50±4.10 | 38.85±3.83 | NS |
| UPDHmm | 21.90±2.06 | 22.43±2.70 | NS |
| LPDHmm | 28.33±3.19 | 27.52±3.29 | NS |
*P<0.05; **P<0.01, NS: Indicates not significant, P>0.05, SD: Standard deviation
Table 4:: Cephalometric values of treatment changes and observation changes (T1–T0) for treated and untreated control groups.
| Measurement | Treated | Control | P value (T1–T0) |
|---|---|---|---|
| Mean±SD | Mean±SD | ||
| SNA° | 0.48±0.51 | 0.54±0.42 | NS |
| SNB° | 1.36±0.82 | 0.59±0.50 | * |
| ANB° | −0.88±0.59 | −0.05±0.08 | * |
| A-Nperpmm | 0.13±0.16 | 0.16±0.15 | NS |
| Pg-Nperpmm | 1.53±0.63 | 0.60±0.65 | * |
| SN-MP° | 0.64+0.17 | −0.08±0.41 | NS |
| FMA° | 0.65±0.28 | 0.02±0.33 | NS |
| LFHmm | 3.70±1.26 | 1.46±0.96 | ** |
| U1-NA° | −0.73±0.81 | 0.31±0.28 | NS |
| U1-NAmm | −0.77±0.86 | 0.11±0.09 | NS |
| L1-NB° | 1.67±2.35 | 0.17±0.13 | NS |
| L1-NBmm | 0.62±1.28 | 0.12±0.10 | NS |
| U1-L1° | 1.55±1.61 | −0.27±1.08 | NS |
| U1-PP° | −0.68±0.89 | 0.28±0.60 | NS |
| L1-MP° | 1.56±2.43 | 0.31±0.21 | NS |
| Overjetmm | −2.19±0.85 | 0.07±0.12 | * |
| Overbitemm | −2.67±0.56 | −0.01±0.06 | * |
| COSmm | −2.83±0.37 | 0.08±0.15 | * |
| UADHmm | 1.05±1.10 | 0.69±0.80 | NS |
| LADHmm | −0.06±0.42 | 0.52±0.34 | * |
| UPDHmm | 0.86±0.74 | 0.44±0.36 | NS |
| LPDHmm | 1.83±1.74 | 0.46±0.42 | * |
*P<0.05; **P<0.01, NS: Indicates not significant, P≥0.05, SD: Standard deviation
DISCUSSION
Deep bite in some Class II short-faced patients may be successfully corrected by cervical pull headgear to extrude the upper molars.[5] On the other hand, the cause of short- face can be from a decreased posterior dental height. When excessive COS is present, extrusion of the lower posterior teeth will improve the lower facial height and correct the COS simultaneously. Clinically, the COS is determined by the distal marginal ridges of the most posterior teeth in the arch and the incisal edges of the central incisors.[19] However, to determine the COS in this study, the measurement did not include the lower second molars as the reference because these teeth had not fully erupted in all subjects. Hence, the first molars were used for measurements in all subjects. Therefore, the depth of the COS was less when compared with other studies that used the distobuccal cusp of the mandibular second molar as a reference.[21]The findings of this study showed that excessive COS was successfully reduced from 3.46 mm to 0.63 mm while the COS in the control group remained unchanged. COS reduction was mainly achieved by extrusion of the posterior teeth (1.83 mm) while anterior tooth intrusion was 0.06 mm. However, the posterior tooth extrusion could be attributed to both extrusive force from orthodontic treatment and dentoalveolar growth. To identify the true treatment changes, measurements of dentoalveolar growth in the untreated control group were applied to the resultant dimensions of the treatment group. Lower posterior dentoalveolar growth in the control group was 0.46 mm; therefore, the net extrusion from treatment was 1.37 mm. The lower anterior teeth in the control group erupted 0.52 mm. Therefore, relative to the control, the anterior teeth in the treated group actually intruded 0.58 mm.
After deduction of dentoalveolar growth, posterior tooth extrusion (1.37 mm) was still greater than the anterior tooth intrusion (0.58 mm). These findings differed from previous COS leveling studies where anterior tooth intrusion was greater than posterior tooth extrusion.[18,21] The conflicting results could be due to different treatment mechanics, especially the posterior vertical elastic that was applied in this study to enhance extrusion of the posterior teeth.
Posterior tooth extrusion was accompanied by favorable vertical skeletal changes in the treated group. The lower anterior facial height in the treatment group significantly increased (3.70 mm) compared to the control group (1.46 mm). This was due to greater posterior extrusion from treatment. The findings were similar to those of a deep overbite correction study by Parker et al.[13] in which the lower facial height increased by 4.04 mm. Likewise, a study by McDowell and Baker[22] found that the lower facial height increased by 3.2 mm. In both studies, upper and lower posterior teeth were extruded. Increases in the lower facial height were related to lower posterior tooth extrusion which was also noted by Weiland et al.,[23] however, that study investigated adult patients.
The mandibular opening rotation was a concern due to posterior tooth extrusion while the lower facial height increased. Despite the fact that significant posterior extrusion occurred in the treatment group, this did not result in a significant opening rotation of the mandible. In this study, the upper and lower posterior extrusion was 0.86 and 1.83 mm, respectively, but the mean increase in the mandibular plane angle was only approximately 0.6°. This was similar to previous studies[22,24] which found that growing patients were able to maintain or had small changes in their mandibular plane angles after deep bite correction. This small amount of opening rotation during posterior extrusion may be explained by compensatory vertical growth of the condyle.[10]
When mandibular opening rotation occurs, the Class II skeletal relationship could worsen. However, there was significant improvement in the maxillomandibular relationship in the treatment group that resulted in a decrease in the ANB angle (0.88°). This improvement contributed to a forward position of the mandible which exhibited a 1.36° increase in the SNB angle and 1.53 mm in Pg-Nperp. This improvement could be explained by the forward growth of the mandible in hypo- and normodivergent pattern patients. This was in agreement with a previous study in which forward growth of B-point in patients with mesofacial and brachyfacial type was also observed.[14] This could be attributed to a forward position of the mandible after unlocking of the bite and allowing forward growth of the mandible.[25] Although the increase in SNB was small, it might encourage a mild Class II skeletal relationship into a Class I relationship. In this study, three of the 22 subjects improved into a Class I skeletal relationship.
In spite of the opening rotation of the mandible, a decreased overjet was observed. Since there was very little alteration in the inclination and position of the incisors during treatment, the reduction of overjet was possibly due to the forward positioning of the mandible together with growth.[25] This was supported by previous studies that found forward positioning of the mandible.[14,18] Unfortunately, however, an overjet measurement was not included in those studies. In the current study, the deep overbite was also improved as a result of lower anterior tooth intrusion and the opening rotation of the mandible.
Usually, when a COS is leveled, lower incisor proclination can be expected since the intrusive force is applied labially to the center of resistance of the lower incisors. Several investigators have reported proclination of the lower incisors to varying degrees when using a continuous archwire.[21,26,27] In this study, lower incisor proclination was found to be approximately 1.5°, but this change was not statistically significant. This value was lower than in previous studies.[21,26,27] This may be due to the step bends on rectangular archwires for COS leveling which produced a counter-clockwise moment to the anterior teeth. Furthermore, cinching the wire may have played a role in preventing the tendency of the teeth to tip labially.[28]
CONCLUSIONS
Increase of the lower facial height in Class II deep bite short-faced patients was successfully accomplished by lower posterior tooth extrusion with the use of rectangular wire and posterior vertical elastics. The mandibular plane angle did not change significantly during treatment. The Class II skeletal relationship improved by forward positioning and growth of the mandible in hypo- and normodivergent pattern subjects who were treated.Financial support and sponsorship
This study was financially supported by the Graduate School and Faculty of Dentistry, Prince of Songkla University, Hat Yai, Songkhla, Thailand.Conflicts of interest
There are no conflicts of interest.References
- Proffit WR, Fields HW, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13:97-106
[Google Scholar]
- Soh J, Sandham A, Chan YH. Occlusal status in Asian male adults: Prevalence and ethnic variation. Angle Orthod. 2005;75:814-20
[Google Scholar]
- McNamara JA. Components of Class II malocclusion in children 8-10 years of age. Angle Orthod. 1981;51:177-202
[Google Scholar]
- Bishara SE. Class II malocclusions: Diagnostic and clinical considerations with and without treatment. Semin Orthod. 2006;12:11-24
[CrossRef] [Google Scholar]
- Henriques FP, Janson G, Henriques JF, Pupulim DC. Effects of cervical headgear appliance: A systematic review. Dental Press J Orthod. 2015;20:76-81
[CrossRef] [PubMed] [Google Scholar]
- El-Dawlatly MM, Fayed MM, Mostafa YA. Deep overbite malocclusion: Analysis of the underlying components. Am J Orthod Dentofacial Orthop. 2012;142:473-80
[CrossRef] [PubMed] [Google Scholar]
- Veli I, Ozturk MA, Uysal T. Curve of spee and its relationship to vertical eruption of teeth among different malocclusion groups. Am J Orthod Dentofacial Orthop. 2015;147:305-12
[CrossRef] [PubMed] [Google Scholar]
- Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62:296-309
[CrossRef] [Google Scholar]
- Burstone CR. Deep overbite correction by intrusion. Am J Orthod. 1977;72:1-22
[CrossRef] [Google Scholar]
- Schudy FF. The control of vertical overbite in clinical orthodontics. Angle Orthod. 1968;38:19-39
[Google Scholar]
- Proffit WR. Contemporary Orthodontics (5th ed). St Louis: Mosby.
- Parker CD, Nanda RS, Currier GF. Skeletal and dental changes associated with the treatment of deep bite malocclusion. Am J Orthod Dentofacial Orthop. 1995;107:382-93
[CrossRef] [Google Scholar]
- Woods MG. Sagittal mandibular changes with overbite correction in subjects with different mandibular growth directions: Late mixed-dentition treatment effects. Am J Orthod Dentofacial Orthop. 2008;133:388-94
[CrossRef] [PubMed] [Google Scholar]
- Chang HP, Kinoshita Z, Kawamoto T. A study of the growth changes in facial configuration. Eur J Orthod. 1993;15:493-501
[CrossRef] [PubMed] [Google Scholar]
- Björk A. Timing of interceptive orthodontic measures based on stages of maturation. Trans Eur Orthod Soc. 1972;6:61-74
[Google Scholar]
- Grave KC, Brown T. Skeletal ossification and the adolescent growth spurt. Am J Orthod. 1976;69:611-9
[CrossRef] [Google Scholar]
- Bernstein RL, Preston CB, Lampasso J. Leveling the curve of spee with a continuous archwire technique: A long term cephalometric study. Am J Orthod Dentofacial Orthop. 2007;131:363-71
[CrossRef] [PubMed] [Google Scholar]
- Braun S, Hnat WP, Johnson BE. The curve of spee revisited. Am J Orthod Dentofacial Orthop. 1996;110:206-10
[CrossRef] [Google Scholar]
- Dahlberg G. Statistical Methods for Medical and Biological Students. London: George Alien and Unwin, Ltd.. 232
[Google Scholar]
- Rozzi M, Mucedero M, Pezzuto C, Cozza P. Leveling the curve of spee with continuous archwire appliances in different vertical skeletal patterns: A retrospective study. Am J Orthod Dentofacial Orthop. 2017;151:758-66
[CrossRef] [PubMed] [Google Scholar]
- McDowell EH, Baker IM. The skeletodental adaptations in deep bite correction. Am J Orthod Dentofacial Orthop. 1991;100:370-5
[CrossRef] [Google Scholar]
- Weiland FJ, Bantleon HP, Droschl H. Evaluation of continuous arch and segmented arch leveling techniques in adult patients a clinical study. Am J Orthod Dentofacial Orthop. 1996;110:647-52
[CrossRef] [Google Scholar]
- Dake ML, Sinclair PM. A comparison of the ricketts and tweed-type arch leveling techniques. Am J Orthod Dentofacial Orthop. 1989;95:72-8
[CrossRef] [Google Scholar]
- Gugino CF, Dus I. Unlocking orthodontic malocclusions: An interplay between form and function. Semin Orthod. 1998;4:246-55
[CrossRef] [Google Scholar]
- AlQabandi AK, Sadowsky C, BeGole EA. A comparison of the effects of rectangular and round arch wires in leveling the curve of spee. Am J Orthod Dentofacial Orthop. 1999;116:522-9
[CrossRef] [Google Scholar]
- Pandis N, Polychronopoulou A, Sifakakis I, Makou M, Eliades T. Effects of levelling of the curve of spee on the proclination of mandibular incisors and expansion of dental arches: A prospective clinical trial. Aust Orthod J. 2010;26:61-5
[Google Scholar]
- Dermaut L, De Pauw GNanda R. Biomechanic aspects of Class II mechanics with special emphasis on deep bite correction as a part of the treatment goal. In: Biomechanics and Esthetic Strategies in Clinical Orthodontics. Philadelphia, PA: WB Saunders. 86-98
[Google Scholar] [Google Scholar]
Show Sections
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου